

The Cost of Doing Nothing Is Already on Your Books

Let's get right to it: poor mental health, suicide risk, substance use disorders, and overdose are already costing your organization — through absenteeism, presenteeism, turnover, disability claims, health care costs, safety incidents, and plain old lost momentum. The question isn't whether this is a business issue. It's whether you're going to address it strategically or keep paying for it quietly.
Depression and anxiety alone cost the global economy approximately $1 trillion annually in lost productivity (WHO, 2022). At the employer level, that shows up in your timesheets, your safety logs, and your exit interviews.
The good news? The return on investment is real — and it's compelling. Investing in mental health at work is the right thing to do, full stop - but it doesn't hurt to know that doing right by your people can also deliver a meaningful return on investment.
$1 In. $4 Back. More If You Start Earlier.

Every $1 invested in scaled-up treatment for depression and anxiety produces a $4 return through improved health and productivity (Chisholm, et al 2016). That's a solid ROI by any CFO's standard.
But here's where it gets even more interesting. The returns are bigger when employers act earlier and more broadly:
6:1 return — Organization-wide culture change and awareness
5:1 return — Proactive early support and intervention
3:1 return — Reactive treatment after distress has already worsened
(Deloitte, 2020)
Translation: downstream treatment matters, but the real money,
and the real impact, is upstream.
Waiting until someone is in crisis is the most expensive strategy of all.
The Three-Level Strategy That Actually Works
The evidence is clear that no single training, app, or awareness month is going to move the needle on its own. What works is a sustained, comprehensive, braided strategy — one that combines all three levels of prevention (LaMontagne et al., 2014):
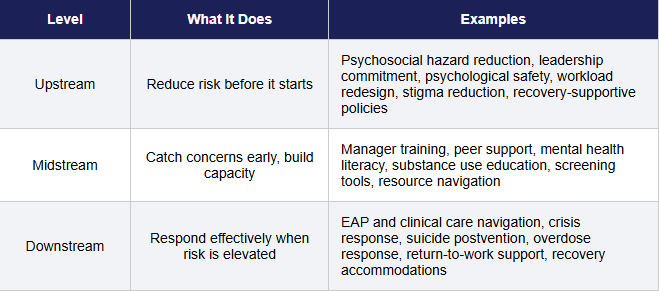
A workplace that only offers counseling after employees are already in crisis will leave money — and lives — on the table. A workplace that only runs resilience workshops without fixing job strain risks blaming workers for conditions the organization has the power to improve.
You need all three levels working together.
Yes, Suicide Prevention and Overdose Prevention Are Part of This Too
This is not a topic to tuck into a footnote. Suicide and overdose are workforce issues — and employers are uniquely positioned to make a difference.
The National Guidelines for Workplace Suicide Prevention (2019) make the case clearly: workplaces that implement safe messaging, crisis response training, and postvention support protect both their people and their organizational stability.
On the substance use side, the National Safety Council (2020) found that employers can save an average of $8500 per employee by supporting workers through treatment and recovery — through reduced turnover, lower replacement costs, decreased absenteeism, and improved productivity. NIOSH and NIEHS (Osborne, et al, 2023) further identify Recovery Friendly Workplace strategies as both a substance use prevention and workplace safety strategy — reducing injury-related pathways to opioid use, decreasing stigma, and supporting workers who are struggling to stay employed and sustain recovery.

Safety Is a Mental Health Strategy (and Vice Versa)
Psychosocial hazards — excessive workload, low job control, bullying, harassment, trauma exposure, and poor supervisor support — don’t just affect morale. They are linked to burnout, psychological distress, injury risk, absenteeism, presenteeism, turnover, reduced productivity, and disengagement. Recent scoping reviews show that poor psychosocial work environments can create cascading effects across worker well-being, safety, and performance outcomes. In healthcare, Amoadu et al. (2025) found that low psychosocial safety climate was associated with poorer working conditions, reduced well-being, and increased safety risks among healthcare providers. Maneen et al. (2025) similarly found that psychosocial work factors — including high demands, low autonomy, poor support, and workplace violence — influenced health, safety, well-being, and productivity among waste collectors.
Li et al. (2024), in a JAMA Network Open systematic review and meta-analysis, found that nurse burnout was associated with poorer patient safety ratings and higher rates of adverse events, medication errors, falls, infections, safety incidents, and missed care.
The evidence is clear: mentally healthy workplaces don't only reduce suffering — they create the conditions for people to do safe, high-quality work. Your safety program and your mental health strategy should be in the same room. Regularly.
The Magic Is Not Automatic — Strategy Beats Random Acts of Wellness Every Time
A 2026 meta-analysis (Backes et al.) confirmed a positive ROI trend across occupational health interventions — while also noting that implementation quality, fidelity, and context matter enormously. In plain English: the money is there, but you have to actually do it well.
A recent systematic review (de Oliveira et al., 2020) found strong evidence that active occupational health involvement reduces mental-health-related sick leave and supports return to work and moderate evidence that workplace-based cognitive behavioral therapy can be cost-saving for depression. Strategy and implementation quality are the differentiators.
Furthermore, the highest returns are unlocked through targeted, multi-component strategies rather than isolated perks. Rigorous economic evaluations confirm that comprehensive prevention and promotion programs are highly cost-effective (Le et al., 2021), especially when they proactively tackle the systemic drivers of presenteeism and psychological injury claims (Yu & Glozier, 2017). When organizations pair these broad cultural shifts with evidence-based clinical support to reduce symptom severity (Joyce et al., 2016) and actively train leaders in supportive, flexible work practices, they achieve causal, measurable improvements in both safety compliance and operational productivity (Hammer et al., 2016). Ultimately, ROI is generated by intentional, systemic design, not superficial, disconnected wellness activities.
The Bottom Line
The return on investment is compelling. The return on inaction is already showing up in your data.
Comprehensive, sustained workplace mental health strategy — one that weaves together mental health promotion, suicide prevention, addiction recovery, and overdose prevention across all three levels of intervention — is both a moral imperative and a sound economic one.
One-off trainings are a line item. A comprehensive strategy is a business investment.

Creating a positive ROI,
Sally
References
Amoadu, M., Wuni, A., Musah, A., Sisala, I. M., Abdulai, A.‑M., Chanayireh, L., & Nyarko, B. A. (2025). Examining the impact of psychosocial safety climate on working conditions, well‑being and safety of healthcare providers: A scoping review. BMC Health Services Research, 25, Article 12254. https://doi.org/10.1186/s12913-025-12254-2
Backes, J., Mueller, S. I., Geissler, A., & Ehlig, D. (2026). Occupational health interventions’ impact on absenteeism and economic returns: A systematic review and meta-analysis. Scandinavian Journal of Work, Environment & Health, 52(2), 79–97. https://doi.org/10.5271/sjweh.4265
Chisholm, D., Sweeny, K., Sheehan, P., Rasmussen, B., Smit, F., Cuijpers, P., & Saxena, S. (2016). Scaling-up treatment of depression and anxiety: A global return on investment analysis. The Lancet Psychiatry, 3(5), 415–424. https://doi.org/10.1016/S2215-0366(16)30024-4
Deloitte. (2019). The ROI in workplace mental health programs: Good for people, good for business: A blueprint for workplace mental health programs. https://www.deloitte.com/ca/en/services/consulting/analysis/mental-health-roi.html
Deloitte. (2020, January 6). Mental health and employers: Refreshing the case for investment. Deloitte UK. https://www.deloitte.com/uk/en/services/consulting/research/mental-health-and-employers-refreshing-the-case-for-investment.html
de Oliveira, C., Cho, E., Kavelaars, R. A., Jamieson, M., Bao, B., & Rehm, J. (2020). Economic analyses of mental health and substance use interventions in the workplace: A systematic literature review and narrative synthesis. The Lancet Psychiatry, 7(10), 893–910. https://doi.org/10.1016/S2215-0366(20)30145-0
Hammer, L. B., Johnson, R. C., Crain, T. L., Bodner, T., Kossek, E. E., Davis, K., Kelly, E. L., Buxton, O. M., Karuntzos, G., Chosewood, L. C., & Berkman, L. (2016). Intervention effects on safety compliance and citizenship behaviors: Evidence from the Work, Family, and Health Study. Journal of Applied Psychology, 101(2), 190–208. https://doi.org/10.1037/apl0000047
Joyce, S., Modini, M., Christensen, H., Mykletun, A., Bryant, R. A., Mitchell, P. B., & Harvey, S. B. (2016). Workplace interventions for common mental disorders: A systematic meta-review. Psychological Medicine, 46(4), 683–697. https://doi.org/10.1017/S0033291715002408
LaMontagne, A. D., Martin, A., Page, K. M., Reavley, N. J., Noblet, A. J., Milner, A. J., Keegel, T., & Smith, P. M. (2014). Workplace mental health: Developing an integrated intervention approach. BMC Psychiatry, 14, 131. https://doi.org/10.1186/1471-244X-14-131
Le, L. K.-D., Esturas, A. C., Mihalopoulos, C., Chiotelis, O., Bucholc, J., Chatterton, M. L., & Engel, L. (2021). Cost-effectiveness evidence of mental health prevention and promotion interventions: A systematic review of economic evaluations. PLOS Medicine, 18(5), e1003606. https://doi.org/10.1371/journal.pmed.1003606
Li, L. Z., Yang, P., Singer, S. J., Pfeffer, J., Mathur, M. B., & Shanafelt, T. (2024). Nurse burnout and patient safety, satisfaction, and quality of care: A systematic review and meta‑analysis. JAMA Network Open, 7(11), Article e2443059.
Maneen, S., Botha, N. N., Amoadu, M., & Ansah, E. W. (2025). Psychosocial work factors influencing health, safety, well-being and productivity of waste collectors in developing countries: A scoping review. BMC Psychology, 13, Article 885. https://doi.org/10.1186/s40359-025-03251-5
National Action Alliance for Suicide Prevention. (2019). National Guidelines for Workplace Suicide Prevention. Workplace Suicide Prevention. https://workplacesuicideprevention.com/wp-content/uploads/2019/10/National-Guidelines-Report.pdf
Osborne, J. C., Chosewood, L. C., Weingarten, A., Rosen, J., & Beard, S. (2023, August 7). NIEHS and NIOSH explore the expansion of recovery friendly workplace programs. NIOSH Science Bulletin, Centers for Disease Control and Prevention. https://www.cdc.gov/niosh/bulletin/2023/friendly-workplaces.html
National Safety Council. (2020). New analysis: Employers can save average of $8,500 for supporting each employee in recovery from substance use disorder. https://www.nsc.org/newsroom/new-analysis-employers-stand-to-save-an-average-of
World Health Organization. (2022). WHO guidelines on mental health at work. World Health Organization. https://www.who.int/publications/i/item/9789240053052
Yu, S., & Glozier, N. (2017). Mentally healthy workplaces in NSW: A return-on-investment study. SafeWork NSW. https://www.nsw.gov.au/sites/default/files/2021-08/nsw-mentally-healthy-workplaces-return-on-investment-study-2017.pdf